Who would ever imagine that
sifting through someone else’s
garbage might create a ruckus.
But that’s exactly what happened <mark style=”background-color:#fff59d”>when</mark>
EXECUTIVE toured Saida’s medical facilities.
Syringes, used blood bags, tubes and IVs lay
loose and in untied bags in the bin behind
Dalaa Hospital. At Labib Medical Center,
syringes and medical gloves littered the
ground, while needles poked out of bags
inside the bin in the parking lot across the
road. There, after just one photo, hospital
security <mark style=”background-color:#fff59d”>showed</mark> up and a scuffle ensued
over the camera. After extracting the security
from the car door, the photographer and driver sped away, while this reporter ran
behind. A third, Hammoud Hospital, transported
its own waste to the city dump.
Strikingly, one of the scavengers who
inhabit Saida’s dump found the contents of
those bags too much to stomach.
Unfortunately, this is an all too common
example of how medical refuse is dealt with
in Lebanon. In the absence of any proper
national policy or waste management system,
hospitals are left to do what they will or can
within their own means. Of Lebanon’s
160 hospitals about 80% are private, with the
majority relatively small in size. That fact
alone could make enforcing a certain code of
conduct difficult. A full 75% of hospitals do
not even know how much waste they generate,
according to a nationwide survey carried
out by Dr Rita Karam, who has a PhD in
hospital waste management. Hospital risk
waste, which requires separate treatment,
includes such things as body parts, infected
materials, syringes, chemicals, radioactive
material and pharmaceuticals. Issa
Consulting and UK-based Environmental
Resource Management (ERM), <mark style=”background-color:#fff59d”>who</mark> are
working as consultants for the government,
estimate that out of a total 20,000 tons of hospital
refuse a year, about one-fifth can be considered
risk waste. That’s tiny compared to the overall daily volume of 3,000 to 3,500
tons of municipal waste. “It’s not the
amount, but the way that it’s handled and
treated that’s dangerous,” says Alissar
Chaker, environmental specialist with Issa.
“The problem is that when [the risk waste]
isn’t segregated it contaminates other waste
streams.” Some 73% of hospitals surveyed by
Karam responded that they do segregate risk
waste, while Dr Faouzi Adaimi, president of
the Syndicate of Hospitals of Lebanon,
claims that all practice segregation. “But still
you need to know if the segregation is done
properly,” says Karam. “Even if hospitals do
practice segregation, they don’t have an ideal method of disposal.” Segregation
should be practiced at each stage of storage,
transportation and treatment as well as
involve proper packaging and labeling.
Some hospitals don’t even have a budget or
waste officer responsible to follow the issue.
Currently <mark style=”background-color:#fff59d”>there</mark> is no regulation governing
how hospitals should manage their waste,
says Naji Kodeih, toxicology specialist
with the ministry of environment. “The
hospitals do what they want. In some
instances there is partial good practice,” he
says, naming the American University
Hospital and Hotel Dieu as examples.
“Partial good practice, but not complete.
This is not bad considering the prevailing
conditions in Lebanon.” But for some that is
simply not acceptable. Zeina Al-Hajj, who
heads the Lebanon chapter of Greenpeace,
refers to the situation as “complete chaos.”

When the old state-owned incinerators
were shut down in 1997, most medical
centers were no longer able to dispose of
their waste in this way. Meantime Sukleen,
which covers greater Beirut and Mount
Lebanon, refuses to collect medical waste
as it is only equipped to handle domestic
waste. “Instead of <mark style=”background-color:#fff59d”>hospitals</mark> investing in
clean technology since then, they have
continued with the same technology,” says
Al-Hajj. Some hospitals have their own
incinerators, but the conditions of those
are questionable due to the lack of control
and their location in residential areas. AUH
acknowledges that its current incinerator is
not suitable, but considers it the lesser of
several evils.
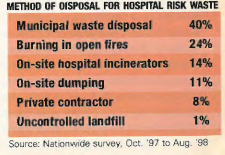
Karam’s survey found that just 14% of
hospitals incinerate their risk waste (see
chart). A large portion is disposed of
through the municipal waste system or by
burning in open fires. Illegal dumping has
been a problem, as has disposal through private
contractors. In many cases it is anybody’s
guess exactly where the waste ends
up. Some claim that medical waste also
finds its way into Sukleen bins regardless of
the company’s stance. “There’s no way we
should accept that medical waste is mixed
with domestic waste in the streets of Beirut
or Lebanon,” says Sarni Rizk, director general
of Rizk Hospital. But according to
Adaimi, most hospitals do sterilize <mark style=”background-color:#fff59d”>their</mark>
waste before disposal, as the equipment is already available for operating rooms. “It’s
not sufficient, I admit, but it’s not the monstrosity
that it’s made out to be,” he says.
In her study, Karam found that “with some
exceptions, the hospital waste management
situation in Lebanon is very far from being
satisfactory and needs to be reconsidered.”
That’s very similar to the findings of a wide-ranging
report on the state of the Lebanese
environment that was published by the ERM
in 1995. Despite its age, the report is still widely
referred to because of its comprehensiveness
and a general consensus that the situation
has not improved. At the time, ERM noted
that “most of the [hospital] waste generated
is collected and disposed of by municipal collection
systems, carrying serious risk of epidemic
and infection.” Indeed infection can be
spread through medical waste, but the source
of a disease is often difficult to determine.
While acknowledging that preventative
measures would be ideal, Dr Walid Amar,
director general of the ministry of health,
plays down the gravity of the situation. He believes there is unnecessary panic due to the
attention the issue has received, while
Adaimi talks of “psychological pollution”
because of the nature of hospital waste.
“Hospital waste accounts for barely 1% of
hazardous waste,” says Adaimi, pointing to
other sources of waste, such as industrial and
slaughterhouse waste. “It’s exaggerated.”
Regardless, due to its potentially risky
nature, management of medical waste
shouldn’t be left to happenstance. In fact the
issue has been on the table since the early
1990s. About four years ago, the Council for
Development and Reconstruction (CDR)
estimated that implementing a solid waste
management system, including hospital,
would cost $135 million. The ERM-Issa
study on hospital waste was completed in
February 1999. And now the CDR is looking
at implementing separate projects for medical,
slaughterhouse and industrial waste.
The medical waste management project, the
more advanced of the three, will encompass
hospitals, dental offices, pharmacies
and other refuse of a similar nature, according
to Sarni Ferghali, the CDR’s program
coordinator for solid waste management.
The ERM-Issa study proposed a central
incinerator with a capital cost of $8.53 million
and annual operating costs at
$903,000, or $676 a ton. The other option
is thermal disinfection, which would
require a small incinerator for certain
waste. The capital cost is estimated at
$5.58 million, with annual operating costs
at $757,000, or $485 a ton. The creation of
a proper sorting, collection and transportation
system would bump those figures up
higher. The estimated cost to hospitals is $3
to $5 a day per occupied bed, which in all
likelihood would be passed on to the individual.
Adaimi argues that waste management
should be a service covered by the
municipal taxes that hospitals already pay
and that the patient should not be made to
bear the cost. Government officials, however,
counter that convention is for the user
to pay for waste management and that
those generating hazardous waste must be
responsible for its elimination.
But before worrying about the amount of
funding required and who should foot the
bill, the problem will be in building a consensus
between the various parties
involved in the decision-making process.
Though the study concentrated on incineration,
at the request of the CDR, it is still not
clear that it will be the chosen option. The
three parties involved in the decision are at
odds. The ministry of environment wants an
incinerator that burns at a higher degree than
the one proposed, while the ministry of health favors thermal disinfection.
Proponents of the latter say it makes dealing
with risk waste possible at the hospital
level with smaller equipment, eliminating
the need for a separate collection system and
the air pollution associated with incinerators.
On the other side of the fence, Kodeih
points to the fact that <mark style=”background-color:#fff59d”>thermal</mark> disinfection is not sufficient for about 6% to 8% of risk
waste, which must be incinerated.
Incineration is generally viewed as the
more tried and tested technology, which
has been made cleaner today. But Al-Hajj
criticizes the government’s entire waste
management policy for being based on
incinerators and landfills, whereas the current
world trend is to reduce and recycle
where possible.
Amidst the controversy, some hospitals
have decided to find their own solution. Last
year Rizk Hospital replaced its 40-year-old
incinerator and has begun implementing
waste management protocols in line with
ISO standards in hopes of being certified in
2001. “The idea for a centralized system is
great, but the major hospitals can’t wait
for the government,” says Sarni Rizk, the
hospital’s director general. He’s not alone.
AUH is having a new <mark style=”background-color:#fff59d”>incinerator</mark> assembled
that will meet the standards of the US-based
Environmental Protection Agency.
The hospital had tried to implement thermal
disinfection, but found such small-scale
equipment of the new technology unsatisfactory.
The major hospitals are considering a joint investment to use thermal <mark style=”background-color:#fff59d”>disinfection</mark>
on a larger scale as a temporary measure
until the government plan is implemented,
says Azmi Imad, the director of AUB’s
environmental health and safety.
Eventually the Lebanese authorities will
have to come up with a national solution, as
many hospitals won’t find the funds or the
will to make such investments. Ferghali
says that waste management is a priority
and the CDR is pushing for the three parties
to come to an agreement. “It’s not
always easy because of the NIMBY effect.
People say ‘that’s good, but not in my
back yard.’ But things have started evolving
in the right direction,” he says. Once an
option is agreed upon and financing
secured, Ferghali estimates that the system
will take about 18 months to two years to
implement. In other words, hospital risk
waste will continue to be mismanaged at
least until 2002, and then only if a decision
is made quickly and proper implementation
and control follow. The Lebanese authorities
don’t have a good track record in fixing
what ails this country. So, don’t expect
a miracle cure.
Such a waste
Perhaps the only thing that has saved Lebanon from
being turned into an environmental disaster is the fact
that it’s not a highly industrialized country. It certainly
couldn’t be put down to sound management strategies on
the part of the government or individual diligence and care
by all industries. Both of those are sadly lacking. The fact is
that unless polluting industries are forced to stringently abide
by specific regulations, more often than not they won’t.
Discussions on dealing with industrial waste are still ongoing
between the ministries of environment (MOE) and industry,
the municipalities and the Lebanese Industrialists’
Association (LIA), despite the number of reports produced
since the mid 1990s. The ministry of industry and petroleum
produced its own in 1994, ERM followed suit in 1995, while a
massive report was prepared by Dar Al-Handasah and
another by a Dutch consulting firm a couple of years ago.
Anwar Berberi, president of the LIA’s environmental division,
contends that the reports were a waste of time and money as
they were conducted by non-experts and based on some inaccurate
data. Berberi, who has patented his own liquid waste
management system, is angry that this government hasn’t
involved the industrialists or the local experts in the process.
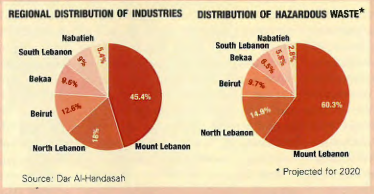
Hazardous waste was estimated at about 18,500 tons a
year in 1994 and projected to increase to 64,500 by 2020, according to the Dar Al-Handasah report. The largest
quantity is forecast for Mount Lebanon (see chart). ” In
Lebanon the quantity is small and the degree of toxicity low,
but there are some compounds in enough quantity to
represent a potential risk for serious pollution,” says Naji
Kodeih, toxicology specialist at the MOE, who estimates
hazardous waste at 10,000 to 15,000 tons.
In general, industries discharge waste with little – if any –
treatment into rivers, lakes, the sea, ground or sewage system,
though Kodeih notes that some of the big industries
do have their own treatment facilities. Berberi agrees, saying
that both liquid waste and hazardous solid waste are
“extremely mismanaged.” Many point to the tanneries as
the worst offenders, because of the heavy metals produced.
Kodeih says the government is working with large
enterprises such as the Lebanese Chemical Company and
Eternit, which still uses asbestos. Cimenterie Nationale
alone has spent $12 million to become more environmentally
sound. There is also a unit within the ministry that is
working on eliminating CFC emissions.
But finding the right fix across the board will not be easy.
Berj Hajian, the MOE’s director general, declined to meet with
EXECUTIVE to discuss delays in finding and implementing a
solution. One problem is the disorganization and distribution
of industry in Lebanon, says Kodeih. “It’s a question of
zoning. You have small industries in residential areas, and a
low awareness among the general population, industrialists
and decision-makers about the hazards of some waste produced.”
Currently there are some 22,000 industrial units scattered
around the country. It is estimated that over 70% are
backyard industries employing less than five people, while
just 2% are considered to be large, employing over 250. The
highest concentration of industry is in Mount Lebanon (see chart). And many industrial units are located outside
designated industrial
zones. There is a proposal
to cluster each type of
industry together so that
they can share the same
infrastructure, including
waste treatment, and
benefit from economies
of scale. But that is still
controversial. According
to Berberi, it’s a question of so many different parties wanting to take control. To
date, nothing has been decided. There are also few recycling
facilities as many have been forced to shut down due to economic
difficulties.
Many raise concerns about the level of pollution in certain
areas. But so far there has been no serious study on the effects
of industrial pollution on the environment or public
health. There is a high level of bronchitis and respiratory
diseases in Chekka and the population is affected immediately
around the plants in Zouk and Sibline, according to
Mutasem El-Fadel, professor of environmental and water
resource engineering at American University of Beirut.
The Dar Al-Handasah report proposed three alternatives
for managing each industrial wastewater, solid waste and air pollution.
It estimated the
national cost at $0.24
per cubic meter of
wastewater and $16.5
per ton of solid waste,
while preferring pre-treatment
of liquid
waste and segregation
of hazardous waste at
the factory. “The problem
in reality is not whether we have standards or not but
the means of implementation, this is the real problem,” says
Kodeih. One problem is financing: The MOE has one of the
lowest budgets of all ministries – it has been allocated just
$2 million this year. But it must be strengthened to act. Until
then, any plans or legislation will just continue to collect dust.